Office Policies / Procedures Signature Pages
Please click on the blue links below, read carefully and sign your acceptance by entering your First and Last Name in the boxes below.
View / Print HIPAA Privacy Policy Form
The final HIPAA privacy rules prohibit the notice and consent from being combined into a single document.
Carolina Family Vision Patient Consent Form
Our Notice of Privacy Practices provides information about how we may use and disclose protected health information about you. You have the right to review our notice before signing this consent. As provided in our notice, the terms of our notice may
change. If we change our notice, you may obtain a revised copy by contacting Carolina Family Vision at (919) 386-2020 or at 504 Village Walk Drive, Holly Springs, NC 27540.
You have the right to request that we restrict how protected health information about you is used or disclosed for treatment, payment or health care operations. We are not required to agree to this restriction, but if we do, we
are bound by our agreement. By signing this form, you consent to our use and disclosure of protected health information about you for treatment, payment and health care operations. You have the right to revoke this consent, in writing,
except where we have already made disclosures in reliance on you prior consent.
Patient Signature:
Date:
NOTICE OF PRIVACY PRACTICES ACKNOWLEDGEMENT
I understand that, under the Health Insurance Portability & Accountability Act of 1996 ( "HIPPA"). I have certain rights to privacy regarding my protected health information. I understand that this information can and will be used to:
- Conduct, plan and direct my treatment and follow-up among the multiple healthcare providers who may be involved in that treatment directly and indirectly.
- Obtain payment from third party payers.
- Conduct normal healthcare operations such as quality assessments and physician certifications.
I have received, read and understand your
Notice of Privacy Practices containing a more complete description of the uses and disclosures of my health information. I understand that this organization has the right to change
its
Notice of Privacy Practices from time to time and that I may contact this organization at any time at the address above to obtain a current copy of the
Notice of Privacy Practices.
I understand that I may request in writing that you restrict how my private information is used or disclosed to carry out treatment, payment or healthcare operations. I also understand you are not required to agree to my requested
restrictions, but if you do agree then you are bound to abide by such restrictions.
Relationship To Patient:
Patient Signature:
Date:
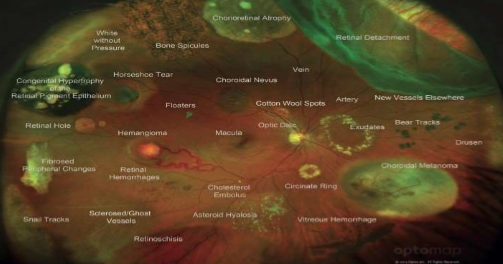
Optomap Retinal Exam
In our continued effort to bring the most advanced technology available to our patients, we have incorporated the Optomap ultra-wide digital retinal imaging and Topcon Maestro OCT retinal scan into your exam today.
The Optomap is a quick, non invasive scan that allows your doctor to see beneath the surface of your retina. The OCT is a quick, non-invasive scan of the retinal layers and optic nerve. OCT uses lightwaves to take cross section
pictures of your retina. The Optomap utilizes scanning lasers to create a high definition image of 90% of the human retina. This unique technology can help our doctors detect vision threatening and systemic diseases in their very early
stages, when they are most treatable.
As part of your pre-testing, our technician will perform the Optomap scan which your doctor will review with you during your examination today. The $39 charge is not covered by your vision insurance or medical insurance, so this
will be added to the balance of your visit.
Normal Wide field retinal image on the Optomap retinal exam.
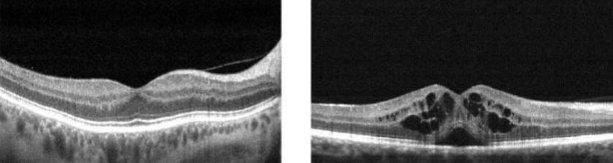
Normal retinal cross section OCT
Diseased retina visible to OCT exam
As part of your examination today, your Doctor needs for you to have an Optos Wide-field Digital image and Maestro OCT Retinal Scan. These images help our doctor view the health of your eye and also monitor for any potential vision
threatening conditions. The digital screening images are only $39 and are not covered by medical or vision insurance. This charge will be added to the balance of your visit.
Patient Signature:
Date:
Carolina Family Vision Office Policies
- Copayments: Payment in full is due at the time of service. We accept cash, check, Visa, Mastercard, American Express, Discover, Care Credit and HSA/FSA cards.
- Returned checksWe will assess a $50 fee for any checks returned by the bank for non-payment.
- Cancellation/ No Show Policy: We ask that you provide us with at least 24 hours notice if you are unable to make your scheduled appointment. Anyone who cancels or does not show up for their appointment within 24 hours will be
assessed a $25 - $50 fee which must be paid prior to being seen in our office.
- Services: During your examination the doctor may request further specialized tests due to medical or family history or to better diagnose any potential eye health problems. In many cases these tests are covered by your major
medical plan. If your plan should not cover the recommended testing these charges will be your responsibility.
For our insurance patients: If you plan to use your insurance as a form of payment you must provide a current id number and insurance information prior to your appointment. If your vision plan is not listed on your
main medical insurance card you must inform us of the vision plan's name so we can research and determine your coverage.
If you have not presented your insurance information prior to the completion of your examination we will not be able to provide refunds, order cancellations or adjustment to fees AFTER services have been rendered and/or your order for glasses and/or contact lenses have been placed.
You may be able to file for reimbursement on your own. If you require a referral for your medical insurance you are responsible for arriving with the referral from your Primary Care Physician. Although we pre-authorize
services and materials prior to your arrival, we are told by your insurance company that they do not guarantee payment of the claim until they have processed your individual claim. If your insurance company declines the claim submitted,
you will be responsible for the balance owed. Please remember, your insurance policy is an agreement between you and your insurance company and not between your insurance company and your provider. Each insurance company has dozens
of plans; all different. It is impossible for our staff to have complete knowledge of each one
- Contact Lens Patients:All Patients wearing contact lenses receive tests and follow-up above and beyond a comprehensive exam. This contact lens medical evaluation is performed every 12 months whether or not new contact lenses
are purchased. Understand there is an additional charge for this service, called a âÃÂÃÂContact Lens EvaluationâÃÂÃÂ. This includes a 90 day window to return at no additional charge if you are having any problems with your contacts. If
you are not doing your contact lens evaluation with us today you have 90 days after your appointment to return to do it. However, if this is your choice we will not be able to dispense any contact lenses to you, write a prescription
for contact lenses, or be responsible for any contact lenses you might continue to wear
- Medical records release/ Forms to be filled out by doctor: We do our best to fill-out necessary forms for schools, DMV etc. and to prepare your records in a timely manner. Please expect 2 business days wait time for them to
be filled out by the doctor and 7 days for finalization of medical records. If your insurance requires prior authorization by provider for prescriptions there will be a $25 processing fee assessed.
We, at Carolina Family Vision want you to be 100 percent happy with your purchase you made with us today. We want you to love your new glasses and will make every effort to stand behind the products we sell. However, because these
are custom products, made just for you, we do not offer refunds.
Signature:
Date: