Please choose from the menu options or
type in your own text. Thank you!
Eye History
Contact Lens Wearers only:
Family Eye History
Does anyone in your family have any of these eye
conditions?
Medical History
Patient & Family Medical History
Does anyone in your family or you have any of these medical
conditions?
Review Of Systems
Social History
Part of a comprehensive visit, we strongly advise the following
procedures:
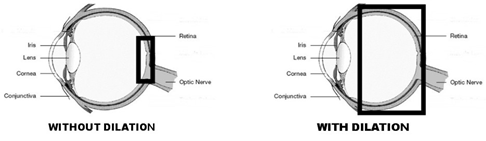
Dilated Fundus Examination
Involves drops to dilate the pupil. Pupil dilation
allows the doctor to examine the entire retina for any signs of disease including
breaks, holes, hemorrhages, tumors or degenerations for which treatment may be
necessary. During routine exams without dilating drops, the pupil size limits the
doctor's view to only the central 30% of the retina. The following diagrams show the
area of retina visible with and without pupil dilation.
The drops take 15 minutes to work and cause the pupil to remain enlarged for about 4
hours. During this time, you will be sensitive to light, and you may have blurry near
vision. Most people can still drive afterwards, although distance vision may be slightly
blurred. We will provide you with disposable sunglasses if you did not bring your own.
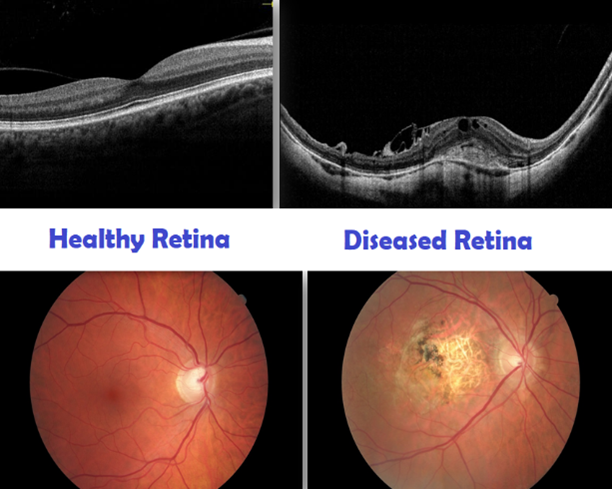
Digital Retinal Imaging
Allows the doctor to get a more magnified view of the internal health of your eye.
• Digital retinal photography uses a specialized camera to take high resolution
images of the back of the eye (retina).
• Optical Coherence tomography (OCT) uses light waves to capture
high-definition 3D views beneath the retina often where signs of eye disease first
appear.
• With the combination of these two tests, images can be tracked and compared
for subtle changes over time.
In refusing dilation, you assume all risks associated with failure to detect eye
conditions due to lack of information that may have been provided by this test. As such,
timely and effective treatment may not be possible resulting in vision loss.
Contact Lens Exam Agreement
(Please only sign if you are scheduled or thinking of having a
contact lens eye exam)
-View Contact
Lens Agreement-
I have read the contact lens patient care agreement and fitting fee. I understand the
fitting procedure and that full payment is expected at the time a contact lens fitting
is performed.
** By entering my First and Last name, I understand, agree
and accept that I am constituting a legally binding electronic signature which I accept has the same validity and meaning as my
handwritten signature.