Digital Retinal Image / Dilation
A DIGITAL IMAGE OF THE RETINA WILL BE DONE ANNUALLY FOR EVERY PATIENT
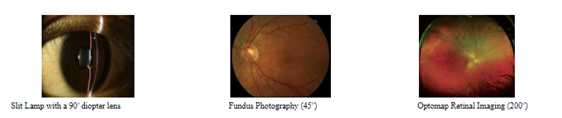
Retinal problems such as macular degeneration, glaucoma, retinal holes, retinal detachments and diabetic retinopathy can now be seen without dilation for most patients and it is far easier for the doctor to examine the eye with the digital image instead of looking through the eye with a microscope which gives a very limited view. The time to evaluate the retina is instant. The exam is painless and allows a 200o view of the entire internal health of the eye without drops.
EARLY DETECTION IS CRUCIAL!!!
Without a thorough internal eye examination serious disease can be missed such as:
All of these can lead to vision loss, blindness or even DEATH.
 The small fee is $29, and may be covered by your insurance company, if a medical condition is found.
The small fee is $29, and may be covered by your insurance company, if a medical condition is found.
"I understand the optos retinal imaging test is the standard of care at Eyeland Vision. This is a required test in order to give the doctors the information they need to give the best quality care for each patient.
Pupil dilation is an important component of every comprehensive eye examination. Along with the Optos, retinal photo, it provides the most adequate view of the inside of your eye and allows your doctor to rule out internal eye diseases, in addition to systemic health conditions.
Dilation involves administering a series of drops into your eyes followed by a waiting period of at least 15 minutes. The side effects include short term blurring of your near vision and increased sensitivity to lights causing some difficulty as it relates to vision while working and or/driving. Some patients find it difficult to drive after being dilated and bring a driver with them.
These effects will last 4-6 hours.
I understand the importance and side effects of having my eyes dilated and I would like to:
Have my eyes dilated today
Reschedule my dilation. There is no additional fee when you return for dilation. (Within 2 weeks)
Not have my eyes dilated today , I understand that my refusal of dilation limits the doctor's ability to detect certain conditions.
Patient Signature
Date