Medical History
CHIEF COMPLAINT
SECONDARY COMPLAINTS:
FAMILY OCULAR HISTORY
Crossed / Lazy:
Retinal Detach:
Macular Degen:
Cataracts:
Glaucoma:
REVIEW OF SYSTEMS:
Do You Currently Have Any Of These Problems?
GENERAL: Fever, weight loss, weight gain, fatigue?
EAR, NOSE, THROAT: Allergies, Sinus, Cough, Dry Mouth / Throat
CARDIOVASCULAR: High BP, Heart Surgery, Vascular Disease
RESPIRATORY: Asthma, Bronchitis, Emphysema, COPD
MUSCLES, BONES, JOINTS: Athritis, Joint Pains, Head or Neck Injury
SKIN: growths, rashes, acne
NEUROLOGICAL: Headaches, migraines, seizures
PSYCHIATRIC: Depression, Anxiety, Insomnia
ENDORCRINE: Thyroid, Diabetes
BLOOD/LYMPH: Anemia, cholesterol, bleeding problems
ALLERGIC / IMMUNOLOGIC: Seasonal Allergies, Rheumatoid, AIDS, Allergy Shots, Lupus
FAMILY MEDICAL HISTORY: Diabetes, HBP, Heart Dz, Cancer, Athritis, Lupus, Kidney, Thyroid, Other
HEIGHT:
FOOT
INCHES
WEIGHT:
POUNDS
TOBACCO:
ALCOHOL:
PREFERRED LANGUAGE:
ETHNICITY:
RACE:
Notice Of Privacy Practices
ACKNOWLEDGEMENT OF RECEIPT OF NOTICE OF PRIVACY PRACTICES
I certify that I have been made aware of Dr. Son and Associates' Notice of Privacy Practices and that I have a right to receive a copy upon request. This Notice describes the type of uses and disclosures of my protected health information that might occur during my treatment, to facilitate the payment of my bills or in the performance of Dr. Son and Associates' health care operations. The Notice also describes my rights and Dr. Son and Associates' duties with respect to my protected health information. I understand that copies of the
Notice of Privacy Practices are available at the front desk. I may request that a copy be mailed to me by calling
703-748-1366
Dr. Son and Associates reserves the right to change the privacy practices that are described in the
Notice of Privacy Practices. I may obtain a revised
Notice of Privacy Practices by calling the above number and requesting a revised copy be mailed to me, by asking for one at the time of my next appointment.
Retinal Photos
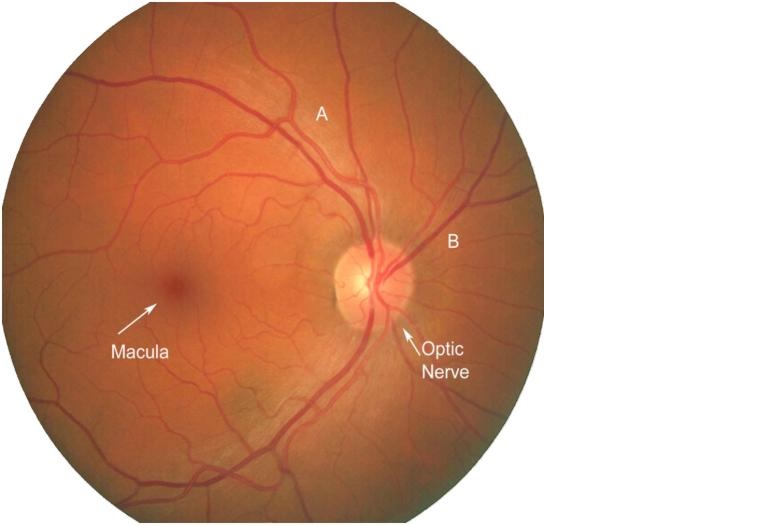
RETINAL PHOTOGRAPHY
A new, highly sophisticated, digital camera now enables us to provide a more thorough retinal analysis of your eyes.
Photo-documentation is painless and in most cases can substitute a dilated examination of your retina.
It can also be an excellent reference point from which future comparison can be made.
Retinal photography can assist us in the early detection of optic nerve disease, pre-cancerous lesions,
macular degeneration, hypertensive retinopathy, diabetic retinopathy, any many other retinal disorders such as
retinal detachment, holes, and thinning.
We strongly recommend that all of our patients receive this test. It is especially important for all people
over the age of 35, as well as those patients who have a history of high blood pressure, diabetes, retinal problems,
headaches, or a strong prescription for glasses.
There is an additional charge of $39 for the retinal photography. Please indicate if you would like to
opt for this evaluation.
Please note: While this test is "optional" for some people as it represents preventative health care,
for others, retinal photo-documentation is "required" because of certain retinal conditions that may be present
or need to be "ruled out." In this latter case, you may be able to submit your bill for the retinal
photography to your major medical insurance company for possible reimbursement.